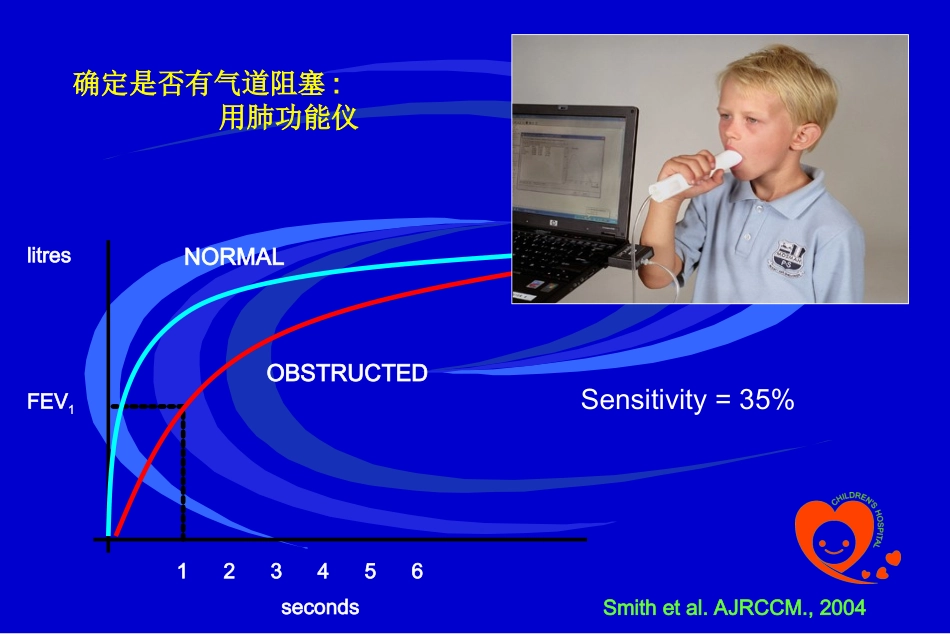
哮喘炎症的非创伤性检测指标及临床意义苏州大学附属儿童医院郝创利AirwaysNarrowing哮喘的病理TriggerfactorMucuspluggingAirwaywalloedemaSmoothmusclespasm确定是否有气道阻塞:用肺功能仪Sensitivity=35%Smithetal
AJRCCM
,2004litresFEV1seconds123456NORMALOBSTRUCTEDGINA哮喘的定义…chronicinflammatorydisorderoftheairways……increaseinairwayhyper-responsiveness……recurrentepisodesofrespiratorysymptoms……variableairflowobstruction……reversiblespontaneouslyorwithtreatment
GlobalINitiativeforAsthma2007ABCDSimpsonetalRespirology2006;11:54-61哮喘的炎症亚型A
NeutrophilicB
EosinophilicC
MixedcellularityD
PaucigranularIsairwayinflammationrelatedto…•cigarettesmoking…
activeorpassive
•infection…
bronchiectasis
•airpollution…
dieselfumes
•allergic(IgE-mediated)asthma
ascarislumbricoides
-Dependingonthecause,thetypeofairwayinflammationmaybedifferent
-Thisisimportantbeca