JNeurosurg74:520-522,1991RemovaloftheroofoftheexternalauditorymeatusinapproachingthetentorialnotchthroughalowtemporalcraniotomyTechnicalnoteMARCP
SINt)OU,M
,ANDJEAN-LucFOBi:,M
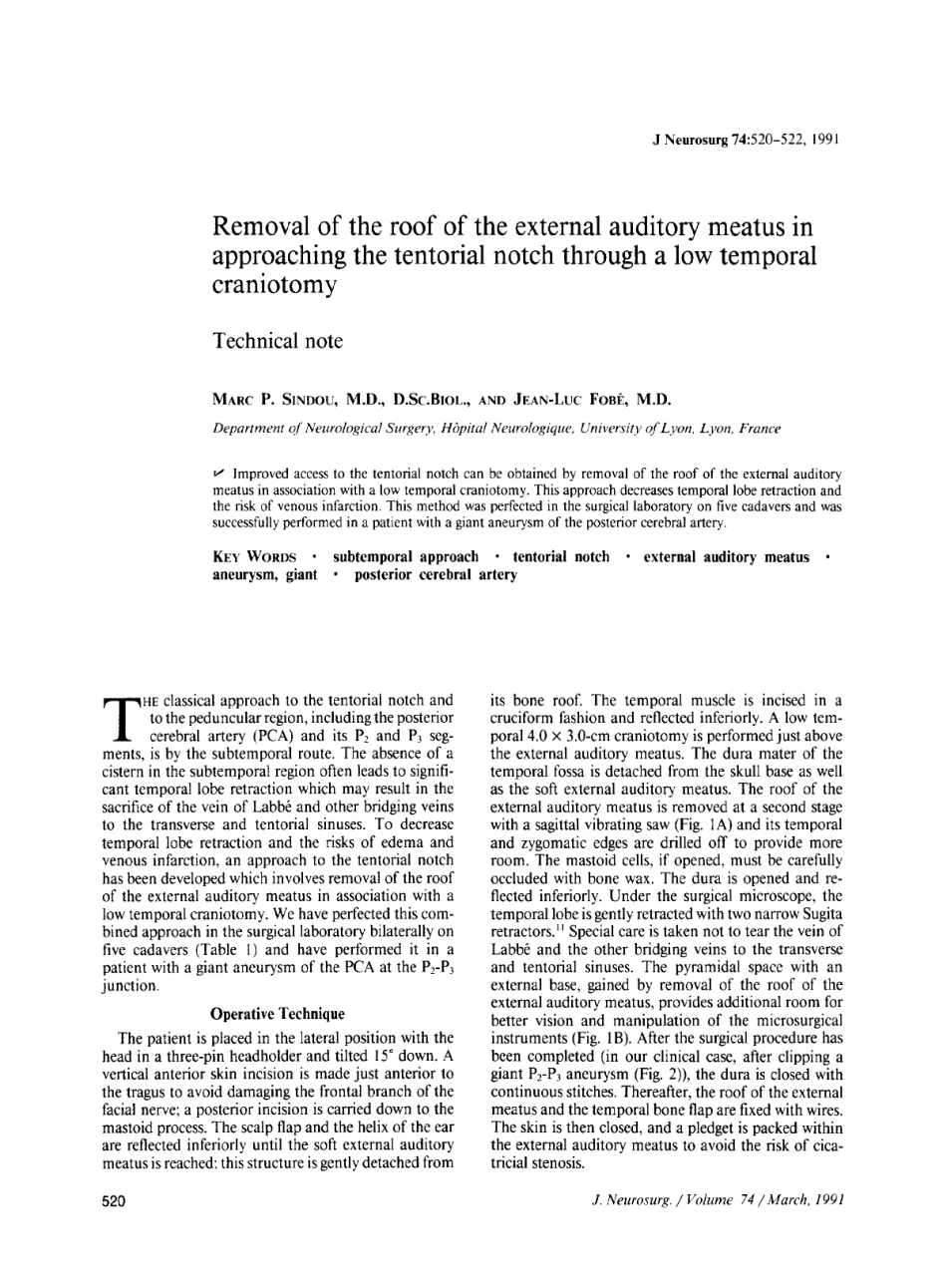
DepartmentofNeurologicalSurgery,HOp#a~Neurologique,UniversityofLyon,Lyon,Franceu-Improvedaccesstothetentorialnotchcanbeobtainedbyremovaloftheroofoftheexternalauditorymeatusinassociationwithalowtemporalcraniotomy
Thisapproachdecreasestemporalloberetractionandtheriskofvenousinfarction
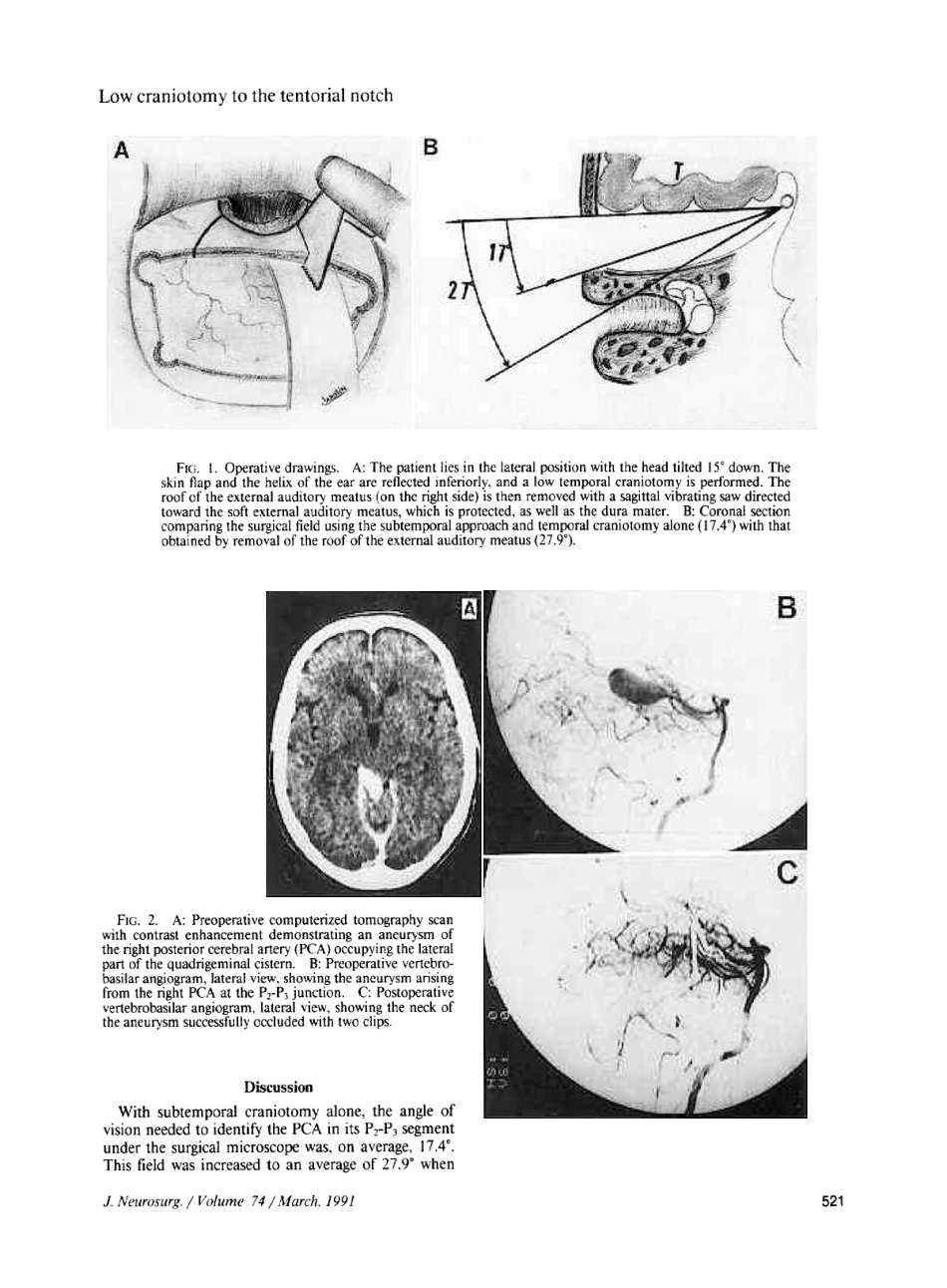
Thismethodwasperfectedinthesurgicallaboratoryonfivecadaversandwassuccessfullyperformedinapatientwithagiantaneurysmoftheposteriorcerebralartery
KEYWORDS'subtemporalapproach9tentorialnotch9externalauditorymeatus9aneurysm,giant9posteriorcerebralarteryTHEclassicalapproachtothetentorialnotchandtothepeduncularregion,incl