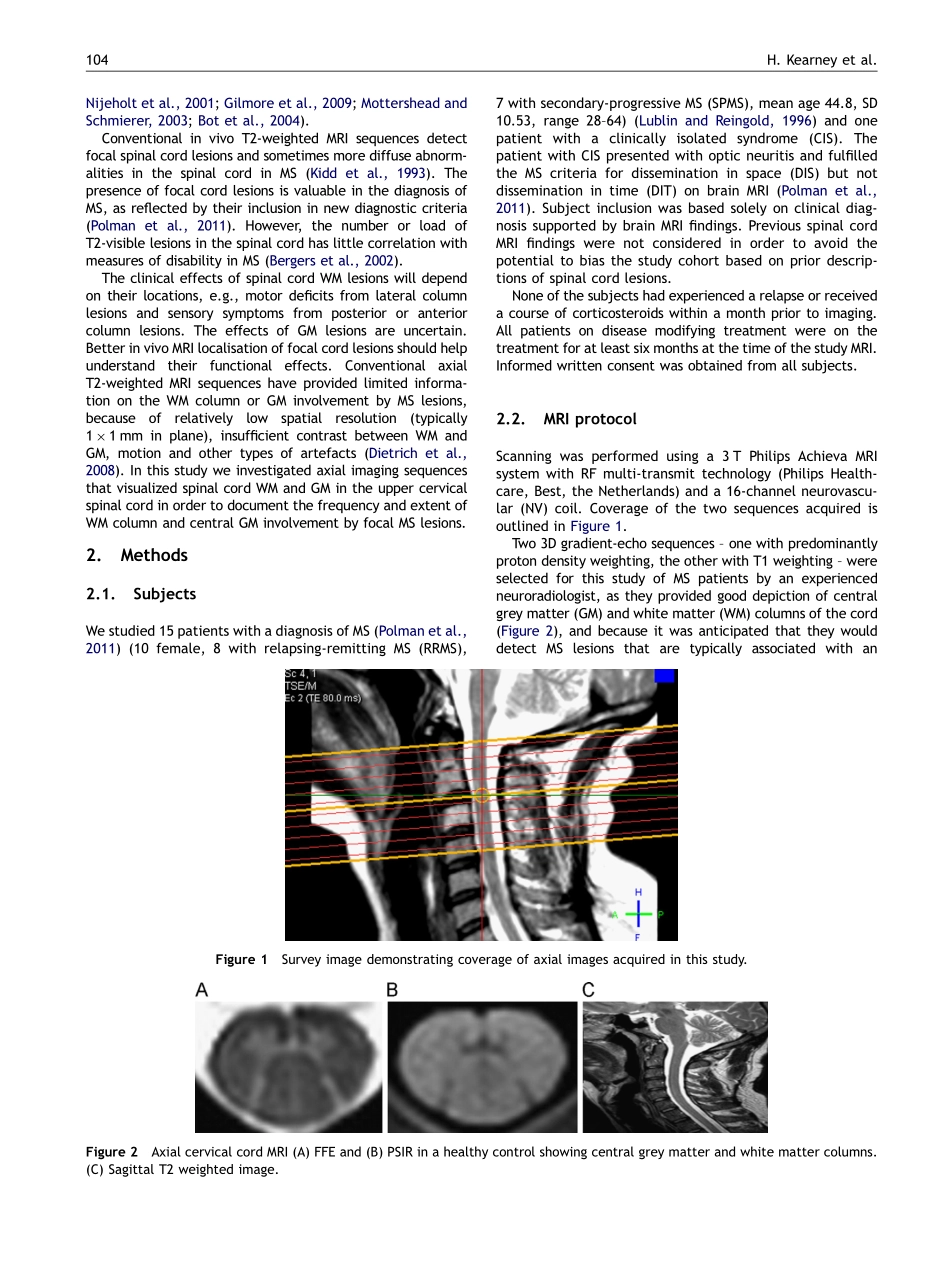
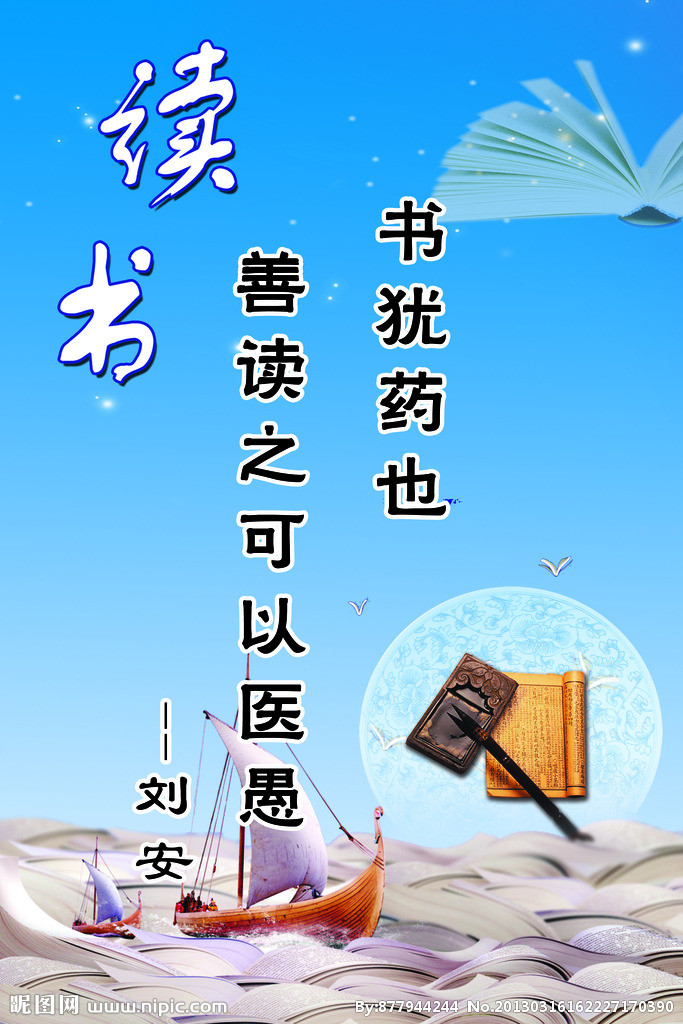
journalhomepage:www.elsevier.com/locate/msardAvailableonlineatwww.sciencedirect.comApilotMRIstudyofwhiteandgreymatterinvolvementbymultiplesclerosisspinalcordlesionsH.Kearneya,n,K.A.Miszkielb,M.C.Yiannakasa,O.Ciccarellia,D.H.MilleraaNMRResearchUnit,QueenSquareMultipleSclerosisCentre,UCLInstituteofNeurology,London,UKbDepartmentofNeuroradiology,NationalHospitalforNeurologyandNeurosurgery,London,UKReceived3July2012;receivedinrevisedform30August2012;accepted12September2012KEYWORDSMultiplesclerosis;Spinalcordlesions;MRI;Whitematter;Greymatter;SpinalcordpathologyAbstractObjectives:Spinalcordpathologyisamajorcauseofdisabilityinmultiplesclerosis(MS)andpathologystudiesshowmultifocaldemyelinatinglesionsinwhitematter(WM)tractsandcentralgreymatter(GM).BetterlocalisationofcordlesionsbyinvivoMRImayhelptounderstandthestructural–functionaleffectsofspinalcordpathologyinMS.Methods:Three-TeslaMRIwasperformedonuppercervicalcordin15MSpatientsandoneclinicallyisolatedsyndrome.Axial3Dgradient-echofastfieldecho(3D-FFE)andphasesensitiveinversionrecoverysequences(3D-PSIR)wereacquired.Tworeadersreviewedimagestodetectandclassifylesions:WM-only,mixedWM–GMorGM-only.LocationoftheWMcomponentwasclassified:anterior(AC),lateral(LC)orposterior(PC)column.Results:Fiftyonelesionswereidentified:32(63)mixedWM–GM,19(37)WM-only,noGM-only.MostwereinLC(n=30,59),followedbyPC(n=18,35)andAC(n=3,6).Meanlesionareas:AC4.3mm2,LC8.5mm2,PC11.3mm2,correspondingto6.1,12and16.1ofmeancordarea,respectively.Meanlesionlengths:18.3mminAC,LC17.6mmandPC24.8mm.Conclusions:WhiletherewasgooddepictionofWMtractinvolvementbycordlesions,involvementofcentralgreymatterwasnotasclear.NotingtheimportanteffectsofspinalcordpathologyinMS,furtherworktobetterdepictcordlesionsbyinvivoimagingiswarranted.&2012ElsevierB.V.Allrightsreserved.1.IntroductionSpinalcordpathologyisamajorcauseofdisabilityinmultiplesclerosis(MS).PathologicalstudiesofthespinalcordinMShavedetailedthemorphologyanddistributionoflesionsdemonstratingwedge-shapedlesionspredominantlyintheposteriorandlateralwhitematter(WM)columns(Fog,1950).Morerecentpost-mortemmagneticresonanceimaging(MRI)andhistopathologicstudieshaveidentifiedadditionalinvolvementofcentralgreymatter(GM)byspinalcordlesions,withbothGM-onlyandmixedWM–GMlesionsbeingdetected(Gilmoreetal.,2006;Lycklama�a2211-0348/$-seefrontmatter&2012ElsevierB.V.Allrightsreserved.http://dx.doi.org/10.1016/j.msard.2012.09.005nCorrespondingauthor.Tel.:+442078373611;fax:+442072785615.E-mailaddress:hugh.kearney.10@ucl.ac.uk(H.Kearney).MultipleSclerosisandRelatedDisorders(2013)2,103–108Nijeholtetal.,2001;Gilmoreetal.,2009;MottersheadandSchmierer,2003;Botetal.,2004).ConventionalinvivoT2-weightedMRIsequencesdetectfocalspinalcordlesionsandsometimesmorediffuseabnorm-alitiesinthespinalcordinMS(Kiddetal.,1993).ThepresenceoffocalcordlesionsisvaluableinthediagnosisofMS,asreflectedbytheirinclusioninnewdiagnosticcriteria(Polmanetal.,2011).However,thenumberorloadofT2-visiblelesionsinthespinalcordhaslittlecorrelationwithmeasuresofdisabilityinMS(Bergersetal.,2002).TheclinicaleffectsofspinalcordWMlesionswilldependontheirlocations,e.g.,motordeficitsfromlateralcolumnlesionsandsensorysymptomsfromposteriororanteriorcolumnlesions.TheeffectsofGMlesionsareuncertain.BetterinvivoMRIlocalisationoffocalcordlesionsshouldhelpunderstandtheirfunctionaleffects.Conventional...