ThyroidCancerShuguangHospitalGeneralSurgeryVINCENTRaoTHYROIDCANCER3whattodowithit
TREATMENT4HOWBADISIT
PROGNOSIS1whereisit
ANATOMY2whydidithappen
ETIOLOGY1
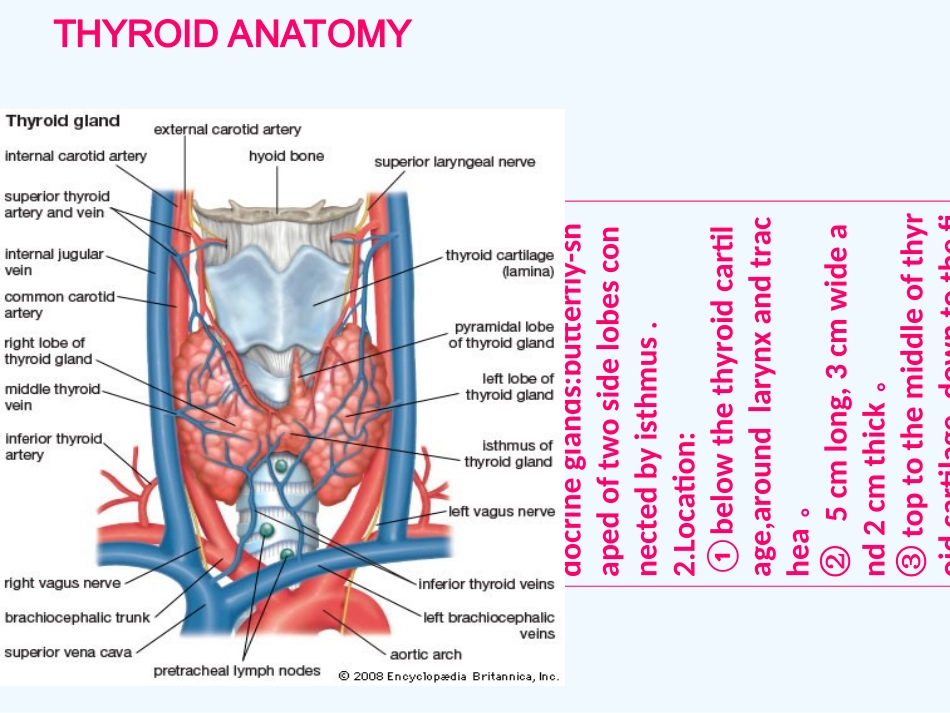
Apperance:thelargestendocrineglands:butterfly-shapedoftwosidelobesconnectedbyisthmus
Location:①belowthethyroidcartilage,aroundlarynxandtrachea
②5cmlong,3cmwideand2cmthick
③toptothemiddleofthyroidcartilage,downtothefifthorsixthtrachealring
THYROIDANATOMY③④Fromskintothyroid:skin→superficialfascia(platysma)→superficiallayerofdeepfascia→infrahyoidmuscles→Pretrachealfascia→thyroidTHYROIDANATOMY③3
Nervesandvessels(bothcoupled):①2nerves:superiorlaryngealnerve+recurrentlaryngealnerve
②2arterys:superiorandinferiorthyroidarterys③3veins:superior、middleandinferiorthyroidveins
Lymphaticdrainage:knowingthewayhowthroidcancercelltransfersisthefound