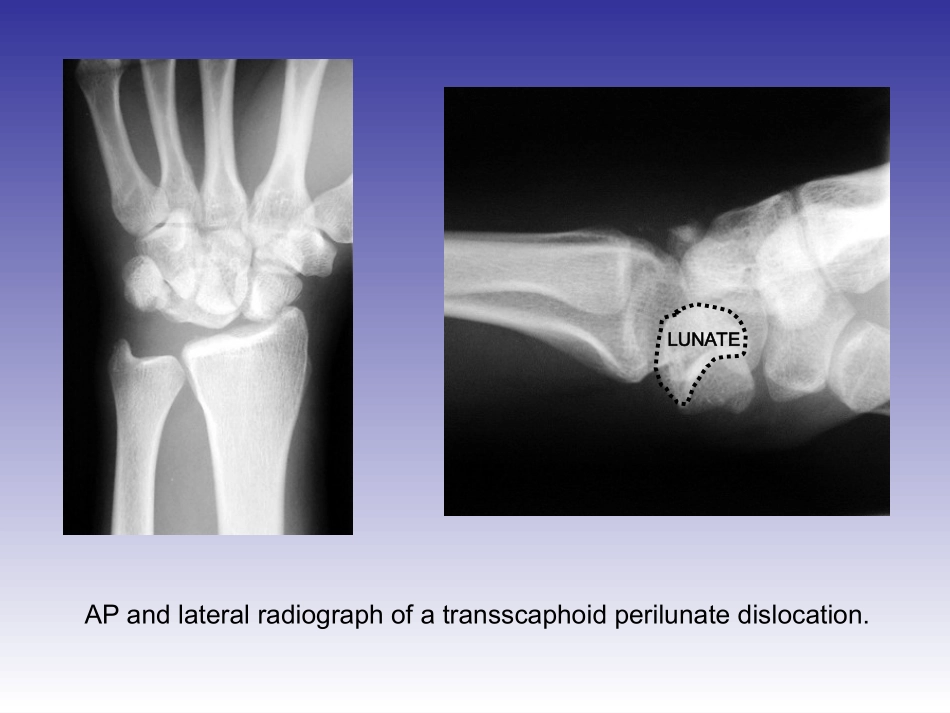
MacintoshPICTimageformatisnotsupportedLUNATEAPandlateralradiographofatransscaphoidperilunatedislocation
Thelunateisfacingdirectlyvolarandislocatedinthecarpalcanal
LUNATECAPITATEAfterattemptatclosedreductionintheemergencyroom,thepatient’slunatewasrepositionedagainstthedistalradius,howeverthemidcarpusisstilldislocatedasthecapitateremainsdorsaltothecapitatefossaofthelunate
LUNATECAPITATEThepatient’sneurologicstatuswasintact,withnormalperipheralnervesensation,including2pointdiscrimination
EPLLISTER’STUBERCLEINCISIONDorsalviewofthewristshowingtheextensorpollicuslongus(EPL)tendon
TheEPLtendonpassesulnarwardofLister’stuberclebeforeanglingtowardthethumb
Theincisionisbasedasseen(betweenthethirdandfourthdorsalcompartment)
EXTENSORRETINACULUMTheincisionisbroughtdownthroughthesofttissueandtheextensorr