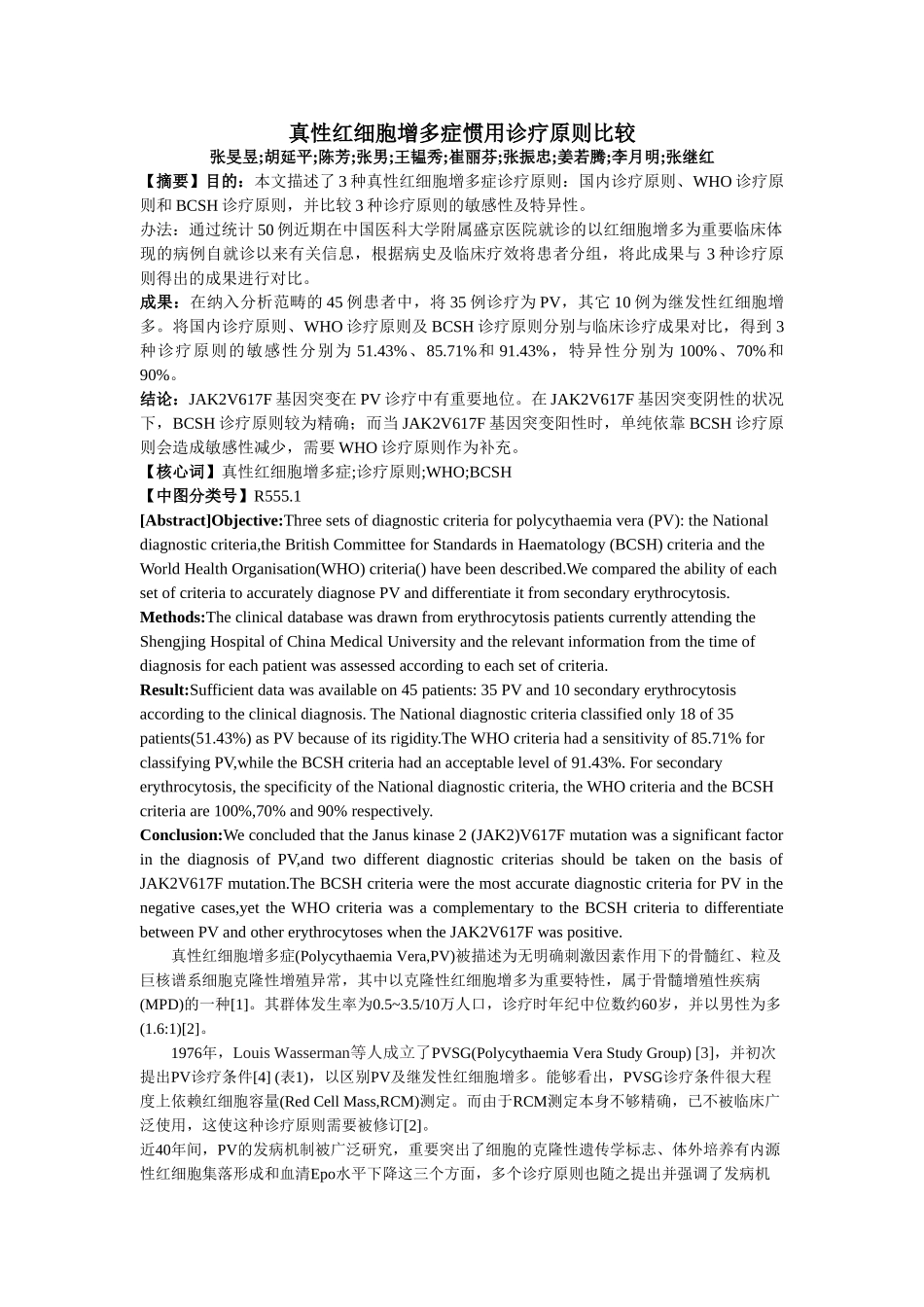
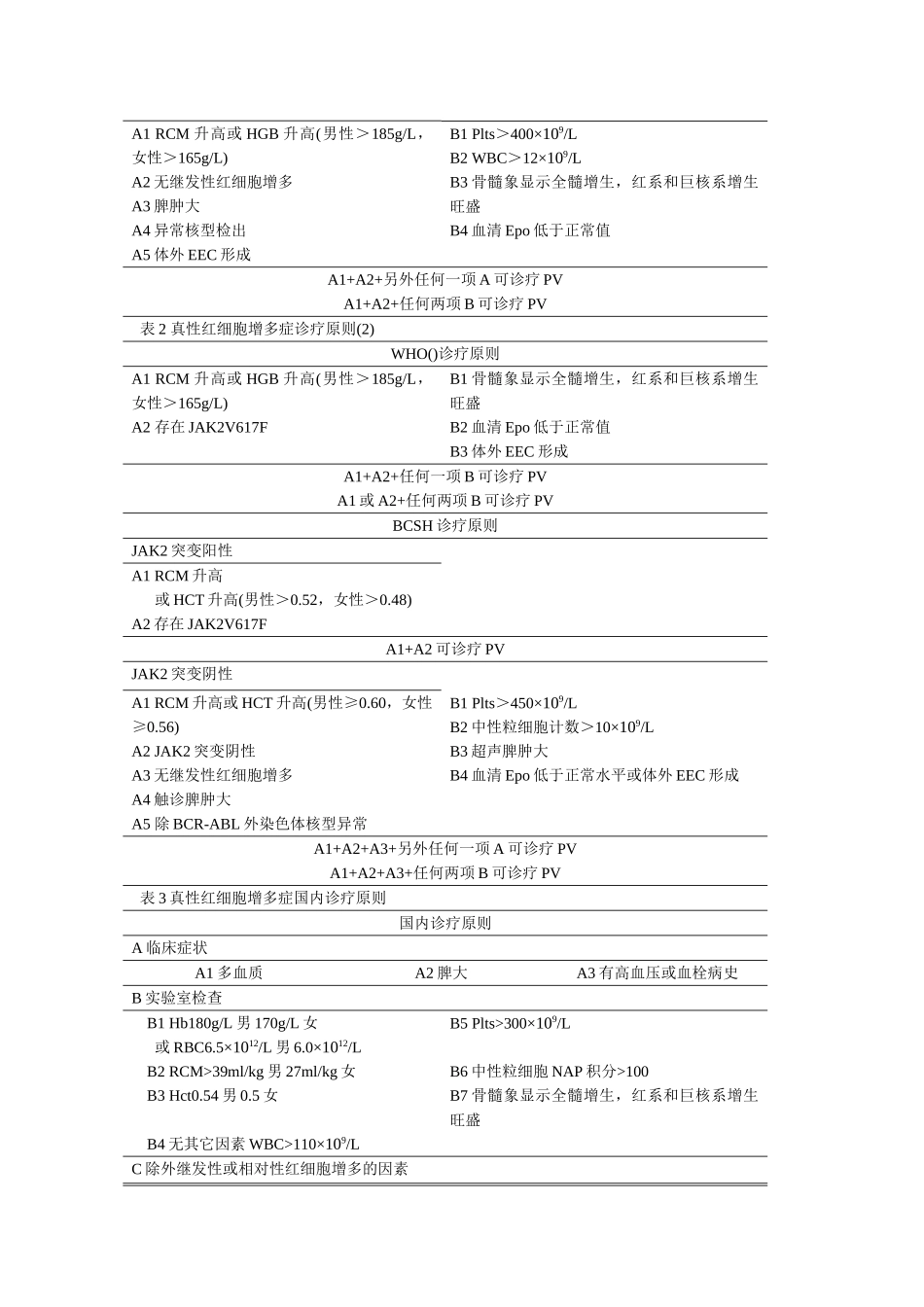
真性红细胞增多症惯用诊疗原则比较张旻昱;胡延平;陈芳;张男;王韫秀;崔丽芬;张振忠;姜若腾;李月明;张继红【摘要】目的:本文描述了3种真性红细胞增多症诊疗原则:国内诊疗原则、WHO诊疗原则和BCSH诊疗原则,并比较3种诊疗原则的敏感性及特异性
办法:通过统计50例近期在中国医科大学附属盛京医院就诊的以红细胞增多为重要临床体现的病例自就诊以来有关信息,根据病史及临床疗效将患者分组,将此成果与3种诊疗原则得出的成果进行对比
成果:在纳入分析范畴的45例患者中,将35例诊疗为PV,其它10例为继发性红细胞增多
将国内诊疗原则、WHO诊疗原则及BCSH诊疗原则分别与临床诊疗成果对比,得到3种诊疗原则的敏感性分别为51
43%、85
71%和91
43%,特异性分别为100%、70%和90%
结论:JAK2V617F基因突变在PV诊疗中有重要地位
在JAK2V617F基因突变阴性的状况下,BCSH诊疗原则较为精确;而当JAK2V617F基因突变阳性时,单纯依靠BCSH诊疗原则会造成敏感性减少,需要WHO诊疗原则作为补充
【核心词】真性红细胞增多症;诊疗原则;WHO;BCSH【中图分类号】R555
1[Abstract]Objective:Threesetsofdiagnosticcriteriaforpolycythaemiavera(PV):theNationaldiagnosticcriteria,theBritishCommitteeforStandardsinHaematology(BCSH)criteriaandtheWorldHealthOrganisation(WHO)criteria()havebeendescribed
WecomparedtheabilityofeachsetofcriteriatoaccuratelydiagnosePVanddifferenti