邱海波东南大学附属中大医院ICU东南大学急诊与危重医学研究所第一页,共四十四页
EarlyvslateCRRT3
Highvsnormalflow4
Possiblewaystoincreasemediatorsclearance第二页,共四十四页
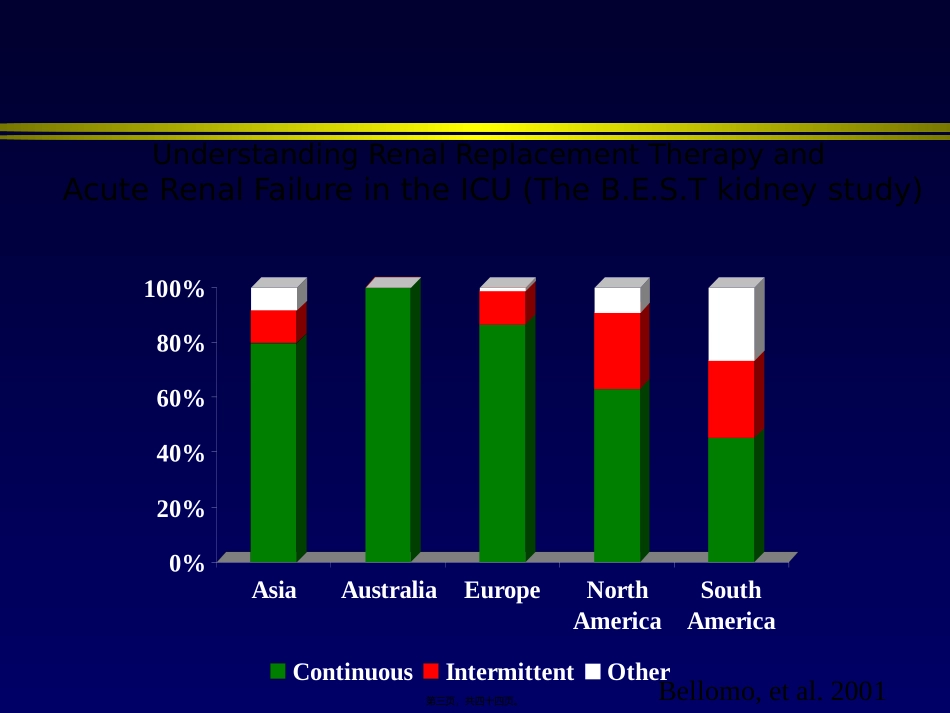
0%20%40%60%80%100%AsiaAustraliaEuropeNorthAmericaSouthAmericaContinuousIntermittentOtherBellomo,etal
2001UnderstandingRenalReplacementTherapyandAcuteRenalFailureintheICU(TheB
Tkidneystudy)第三页,共四十四页
•Retrospectivecohortstudy•PatswithARFandrequireddialysisbetweenApril1,1996,andMarch31,1999•2ICUinCanada
•N=261CRRTIHDPAPACHEII2725
10BaselineSCr1361800
002MAPBeforeRRT74