1、当您付费下载文档后,您只拥有了使用权限,并不意味着购买了版权,文档只能用于自身使用,不得用于其他商业用途(如 [转卖]进行直接盈利或[编辑后售卖]进行间接盈利)。2、本站所有内容均由合作方或网友上传,本站不对文档的完整性、权威性及其观点立场正确性做任何保证或承诺!文档内容仅供研究参考,付费前请自行鉴别。3、如文档内容存在违规,或者侵犯商业秘密、侵犯著作权等,请点击“违规举报”。
碎片内容
邱海波东南大学附属中大医院ICU东南大学急诊与危重病医学研究所ARDS肺复张的实施科学与艺术的困惑第一页,共三十七页
内容提要•肺保护性通气策略不能解决解决的问题•肺泡塌陷的病理生理后果•肺复张的临床实施–Proneposition–Spontaneousbreathing–HighVTandsigh–RM第二页,共三十七页
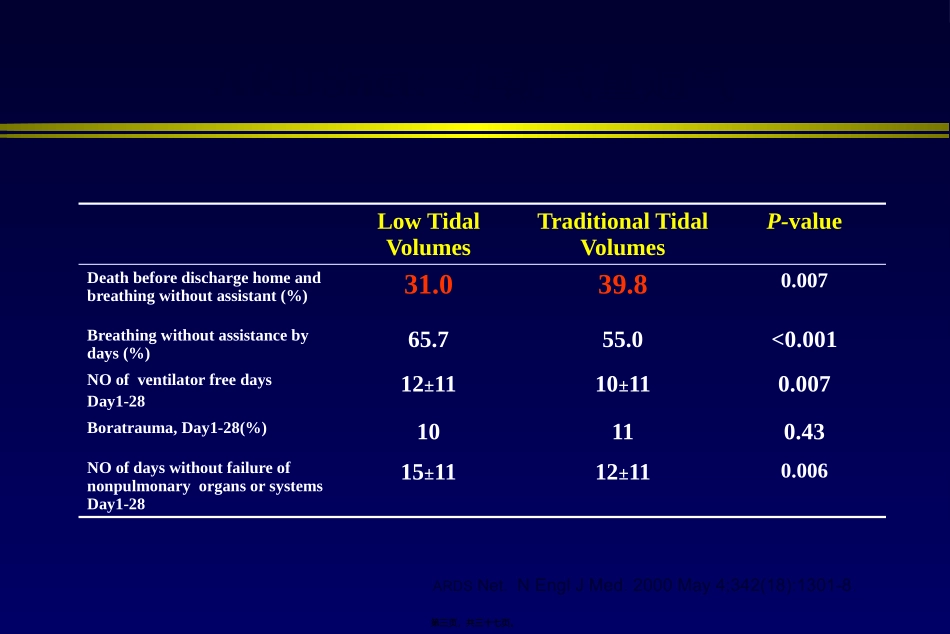
ARDSnet:小潮气量通气LowTidalVolumesTraditionalTidalVolumesP-valueDeathbeforedischargehomeandbreathingwithoutassistant(%)31
007Breathingwithoutassistancebydays(%)65
各种文档应有尽有